A compact week: venture debt fuels vascular access, cardiology gets a non-invasive CE mark, and NICE nudges digital rehab platforms toward the NHS.
People on the move
Lucile Blaise joins LivaNova (UK) as Global Head of Commercialization, Obstructive Sleep Apnea, adding strong EU market access chops to the executive team.
Money flows
Xeltis (NL) gets nearly €50M, venture debt + equity; package includes up to €37.5M from EIB (first €10M drawn) and €10M from existing investors EQT Life Sciences and Invest-NL. Funds push aXess vascular access conduit toward EU commercialization.
Angelini Ventures (Italy): €150M EIB co-investment agreement to back European biotech and digital health startups over six years (EIB €75M + Angelini Ventures €75M). Signals more institutional firepower for EU healthtech.
Annette (France) €2M round to scale its GLP-1 companion care platform for structured obesity support; led by Redstone, Ring Capital and AFI Ventures.
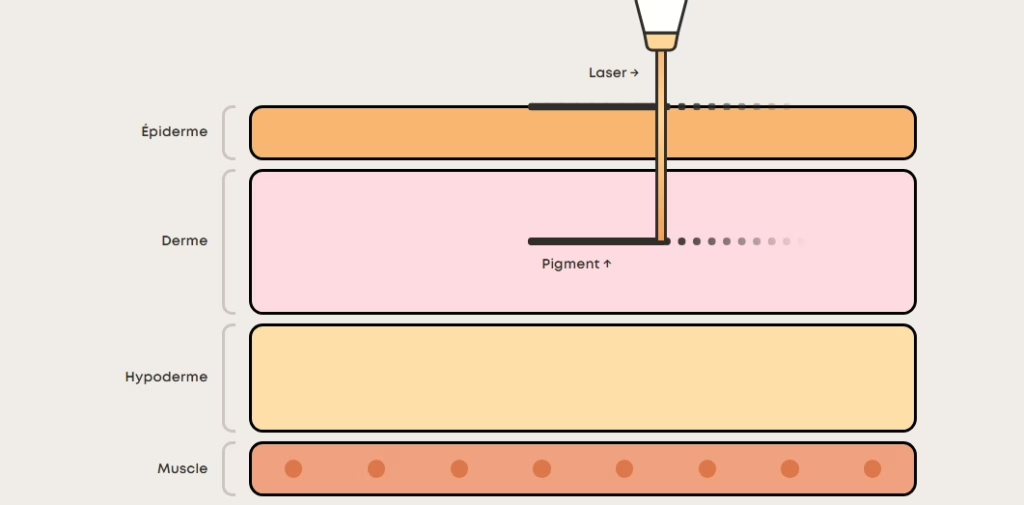
Ray Studios (France) €10M to expand its physician-led tattoo-removal clinic network across Europe; co-led by Factory Capital and Nickleby Capital.
On the press
• Cardiawave (FR): Valvosoft® receives CE Mark as the first non-invasive ultrasound therapy for severe symptomatic aortic stenosis; data cited from EU FIM and pivotal studies across 12 centres.
• Boston Scientific: European approval for the Farapoint™ pulsed-field ablation focal catheter to treat atrial fibrillation, complementing Farapulse™ PFA platform.
• NICE (UK) publishes Early Value Assessment (HTE35) for digital platforms supporting cardiac rehabilitation, enabling conditional NHS use while evidence is generated over three years.
One thing to remember
EU cardiology is having a moment: capital is flowing into commercialization-ready devices, while regulators opened the door to earlier adoption of digital rehab and cleared a novel non-invasive therapy. Founders who can pair strong clinical data with payer-relevant outcomes will find both financing and fast-track pathways this winter.
Robotics bags big money, IVF gets an automation CE mark, and UK regulators sketch next steps for AI in care.
People on the move
Distalmotion (Switzerland) Chas McKhann becomes Executive Chairman alongside a $150M raise; focus is US growth while keeping EU base in Lausanne.
Money flows
Distalmotion (Switzerland) $150M, Series G / growth; scaling DEXTER® surgical robotics with ASC push and US commercial build-out.
Sofinnova Partners (France) — €650M, flagship Capital XI; early-stage focus in medtech/biopharma, active deployment underway.
On the press
• Overture Life (Spain) CE markfor DaVitri™, billed as the first automated device cleared in the EU or US for vitrifying unfertilised eggs; EU commercial rollout begins.
• Cardiovalve (Israel) CE file submitted for transcatheter tricuspid valve after positive TARGET study interim; EU approval process initiated.
• JenaValve (Germany) 1,000th case with CE-marked Trilogy™ TAVR for aortic regurgitation/stenosis, signalling steady EU adoption.
Capital and credibility still move together: big-ticket robotics funding and a heavyweight €650M early-stage fund arrived the same week that EU-relevant CE activity and the UK’s AI-in-health policy guardrails advanced. It is an evidence that clear regulatory paths plus deployment stories are what unlock cheques right now.
The paradigm in healthcare is shifting: instead of “see a doctor when things go wrong”, some start-ups are betting the future lies in “continuous health monitoring for when things haven’t yet gone wrong”. The US model is blazing ahead; Europe is watching with interest and caution.
Strong traction and funding: A beta release in April 2023 reportedly hit ~50,000 paying members and >200,000 on the waitlist. They also closed a Series A backed by top-tier investors including Andreessen Horowitz.
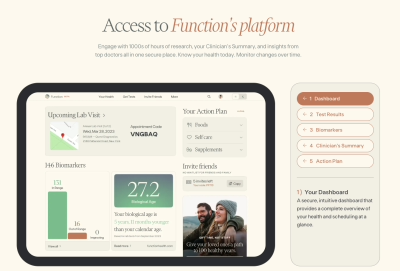
Founded in 2021 (co-founded by Mark Hyman among others) to deliver a membership-based platform offering 100+ biomarker blood tests (and more) twice a year.
Members book tests at lab partners (over 2,000 locations via a partnership with Quest Diagnostics) and then receive reviews and insights from clinicians.
The promise: shift from reactive healthcare (“you’re sick, so treat”) to proactive (“monitor biomarkers, spot trends, intervene earlier”). As described by Function: “Health is not one test — it’s a pattern.”
Why this matters commercially
The business model: subscription + diagnostics + insights. Recurring revenue, high-engagement, measurable service.
The branding is consumer-centric: not “see a doctor”, but “stay ahead of trouble”.
From a marketing/omnichannel viewpoint: digital sign-up, lab booking network, data dashboards, membership renewal incentives.
The value proposition: for individuals willing to pay out-of-pocket, it aligns with performance, longevity, optimisation.
But there are caveats
The price point (~US$499/year for the basic membership) presumes consumers will pay for diagnostics out-of-pocket, outside insurance.
The model thrives in a U.S. environment: high out-of-pocket health spending, fragmented insurance, willingness to pay for wellness. Europe is different.
Europe: Similar plays, but different context
Enter Lucis, a Paris-based start-up positioning itself as “Function Health for Europe”.
Key points:
Lucis offers comprehensive blood testing plus AI-driven insights and personalised recommendations.
They claim to have achieved ~$400k ARR in Paris within four months, partnered with major lab networks in France, and are expanding to multiple European countries.
Their value chain: partner labs (for analytical quality), encrypted GDPR-compliant data, medical team review, actionable results.
Why this is noteworthy for European commercialisation
Reflects an appetite for preventive diagnostics beyond wearable devices and wellness buzz.
Shows that the membership/diagnostics model is crossing the Atlantic, albeit still early stage.
From a marketing perspective: branding preventive health not as gadgetry but as meaningful medical-lifestyle hybrid.
But Europe presents structural challenges
Many European health systems emphasise universal/public coverage; consumer willingness to pay direct for diagnostics may be lower.
Regulatory hurdles: Diagnostic tests often fall under stricter oversight; membership claims around trending biomarkers may invite scrutiny.
Distribution and reimbursement: Selling B2C across countries demands localisation (language, regulatory, lab accreditation) and often B2B or employer channels may be more realistic.
Value proposition needs to show ROI (cost savings, health outcomes) not just “optimisation” for affluent consumers.
Strategic takeaway for life-sciences / omnichannel marketing professionals
If you work in life-sciences commercialisation and are exploring preventive diagnostics or “functional health” (health optimisation, wellness-medical hybrid), here’s a sharper lens:
Model to study: The Function Health structure (subscription + diagnostics + insights) is a template.
Digital marketing to attract consumers or employer channels.
Localise content for markets: language, healthcare system context, pricing comparisons.
Risk management and credibility:
Avoid hype: emphasise what the data can show and what it can’t. Some markers don’t yet have actionable evidence.
Set realistic expectations: diagnostics without follow-through (behaviour change, medical supervision) may be less valuable.
Be prepared for regulatory push-back or scrutiny on claims of “prevention” vs “diagnosis”.
One thing to remember
Subscription diagnostics may be the future’s front door to preventive health, but only those who adapt for Europe’s market dynamics, regulatory terrain and consumer mindset will turn the key.
A compact week: small but pointed rounds in diagnostics and patient safety, a urology partnership scaling across EMEA, radiosurgery planning cleared on both sides of the Atlantic, and a headline corporate restructure.
People on the move
Exstent (UK) – Vascular surgeon Matt Thompson becomes CEO to drive commercialization of patient-specific aortic support.
Money flows
Self.co, formerly known as Allergomedica, (Lithuania) a €2.56M mixed grant + venture to scale molecular allergy testing and expand into the UK, Ireland, Austria and Germany; grant component from Innovation Agency Lithuania.
Enteral Access Technologies (UK) a £500K bridging round to scale DoubleCHEK, its CO₂+pH nasogastric tube placement safety device; building UK adoption and early EU rollout.
Minze Health (Belgium) × Medtronic: a three-year EMEA partnership to offer Minze’s automated bladder diary (Diary Pod) to patients receiving Medtronic sacral neuromodulation therapy; strengthens digital urology care pathways.
On the press
• ZAP Surgical: ZAP-Axon radiosurgery planning system receives both EU CE certification and US FDA 510(k); enables clinical use across the EU and US.
• Siemens to deconsolidate Healthineers: Siemens plans a direct spin-off of 30% of its ~67% stake to shareholders, cutting to ~37% and targeting <20% medium-term; expect governance/strategic autonomy effects for a core European medtech anchor.
Seed-stage cash is trickling into practical, reimbursable workflows (diagnostics, patient safety) while scale comes from channel partnerships and regulatory wins; design for distribution and evidence now so you’re ready when the capital tides turn.
The VCs, public funds, and CVCs writing cheques in European healthtech (2025 edition)
Healthtech funding in Europe is accelerating again. After a cautious 2023, investment rebounded to $4.8 billion in 2024, and Q1 2025 alone brought in $4.3 billion. Healthtech now captures 30 to 35% of all venture activity across the continent. But who’s actually writing those cheques?
This post breaks down the capital stack behind Europe’s digital health growth: venture capital, public funds, and corporate/strategic investors. Whether you’re raising or deploying capital, here’s who you need to know in 2025.
1. Venture Capital: Still the Primary Engine
Venture capital is behind most of the major healthtech rounds in Europe. From seed to Series C, VCs provide the scaling fuel, validation, and network access.
Top 5 VCs Investing in European HealthTech:
Sofinnova Partners: Paris-based life sciences fund active in healthtech, diagnostics, and therapeutics.
Octopus Ventures: UK fund with a strong healthtech thesis, including femtech and digital care.
Speedinvest: Vienna-based early-stage investor with a focus on digital health and care platforms.
EQT Life Sciences: Nordic growth-stage investor in diagnostics, medtech, and health platforms.
Calm/Storm Ventures: Focused on pre-seed and seed-stage digital health across underserved areas like paediatrics and mental health.
Who are the best VCs for digital health in Europe?
Those five are consistently active in 2024-25, spanning early to growth-stage capital.
2. Public & EU Funding: De-risking and Catalysing Growth
Public funding rarely leads rounds, but often enables them. Grants, co-investments, and match funding are key to bridging early clinical stages and reimbursement pilots.
Key Public Funding Sources for HealthTech in Europe:
Horizon Europe: EU R&D programme with dedicated tracks for health and medtech.
EU4Health: €5.3 billion programme for health system resilience and digitalisation.
Bpifrance: France’s national investment bank, active in medtech, digital health, and AI.
Innovate UK: Grant and co-investment body supporting UK healthtech pilots and R&D.
Can you get EU grants for a healthtech startup?
Yes. Programmes like Horizon Europe, EIC Accelerator, and EU4Health fund clinical validation, digital health infrastructure, and medtech scale-up.
3. Corporate Venture & Strategic Investors: Validation with Capital
CVCs and strategic investors are increasingly active in Series B+ deals. They offer more than capital, including access to clinical settings, distribution, and potential M&A.
Key Corporate Venture Funds:
Philips Ventures: Investing in digital diagnostics, patient monitoring, and chronic care.
Do corporates invest in digital health startups in Europe?
Yes. In 2025, CVCs from pharma, medtech, and insurance are increasingly co-investing in digital health.
Estimated Funding Breakdown (2025):
Source
Share Estimate
Role
Venture Capital / PE
65–75%
Lead rounds, scale capital
Public Funds / Grants (EU + National)
10–20%
Early-stage, pilots, non-dilutive
Corporate / Strategic / CVC
10–15%
Strategic fit, late-stage, distribution
Insight: Most healthtech rounds in 2025 involve blended capital: a VC lead, public match-funding, and a strategic partner.
Strategic Takeaways
Founders: Match your capital to your stage. Grants and public co-investments work best pre-revenue or pre-regulatory. Investors: Watch for startups with public funding traction—often a good de-risking signal. Operators: CVCs are gatekeepers to reimbursement and go-to-market. Engage early, but be realistic on timing.
Next up: How the funding mix changed between 2024 and 2025, and what it signals about the future of EU healthtech capital.
The European Commission’s latest 150-page analysis of artificial intelligence deployment in healthcare across the EU isn’t light reading. But it should be mandatory for anyone building or backing AI-driven MedTech. Because while the headlines scream about generative AI revolutionising medicine, the report paints a far less dramatic, but more commercially useful, picture.
This is a story of uneven adoption, promising use cases strangled by red tape, and the growing chasm between regulatory intention and real-world execution. In other words, typical European healthcare.
The Few Use Cases That Work
Despite the hype, only a narrow set of AI applications are actually scaling:
Imaging and diagnostics continue to lead, especially in radiology, pathology, and dermatology. This is due to data abundance and well-defined clinical tasks.
Operational AI is quietly making a difference in logistics and scheduling, especially tools that improve patient flow or reduce no-shows.
Administrative automation using LLMs and NLP is gaining traction, particularly digital scribes and documentation tools.
In all cases, the successful deployments are narrow, specific, and integrated into existing workflows. General-purpose AI or standalone platforms are still a fantasy.
Why Adoption is Stalling
The study outlines 26 distinct barriers. Let’s group the key ones:
1. Data fragmentation and access
Hospitals operate with siloed systems and non-standardised formats. Even when data is available, trust, consent, and governance issues make it unusable.
2. Overlapping regulation
MedTech startups must navigate the AI Act, GDPR, MDR, IVDR, HTA rules, and soon the EHDS. Each imposes its own requirements for transparency, explainability, evidence, and liability.
3. Procurement paralysis
Hospitals rarely procure standalone AI tools. They prefer solutions bundled with existing systems or validated by public-private pilots. That means startups must either integrate into incumbent platforms or navigate years-long public tenders.
4. Lack of robust evidence
Most AI tools lack RCTs or real-world data at scale. This stalls reimbursement and formal adoption. And since HTA bodies treat algorithms like drugs, the evidentiary bar is high and expensive.
5. Cultural resistance
Doctors are wary of black-box tools. Patients aren’t convinced about machine-made diagnoses. And hospital administrators need guarantees, not hype.
Strategic Insights for EU Founders
If you’re a MedTech founder in Europe, here’s what to take away:
Build for integration: Design your AI to plug into Cerner, Epic, or national EHR systems. Standalone platforms won’t survive.
Focus on unsexy wins: AI that reduces admin, improves scheduling, or boosts documentation accuracy is easier to validate and adopt.
Use hospitals as research partners: Academic centres want to publish. Co-develop your real-world evidence with them.
Service, not software: Hospitals want solutions, not licenses. Offer managed services, not just tools.
Treat CE mark as step one: It’s not product-market fit. It’s the starting point for evidence and integration.
What Investors Should Look For
Smart capital should prioritise teams who understand Europe’s slow path to adoption. Key signals include:
Integration-ready architectures
HTA or payer engagement early on
Built-in data governance and local validation
Evidence generation baked into the roadmap
If a startup claims AI disruption without regulatory or clinical depth, pass.
A Final Word
AI in EU healthcare is not a gold rush. It’s a policy-anchored trench war. But for the few who master the terrain, the rewards are durable. Think less blitzscaling, more systems change. Just don’t call it a revolution. In Europe, it’s called compliance.
Every health AI model is a decision engine — and an attack surface.
The Risks (with Evidence)
Adversarial examples derail medical imaging AI — systematic review across radiology (European Journal of Radiology).
Data poisoning, inversion & extraction are recognised clinical AI risks with mitigations like audit trails and continuous monitoring (García-Gómez et al.).
Why Healthcare Is Special
High stakes, legacy networks, and fragile systems — the WannaCry ransomware attack disrupted NHS care at scale (UK National Audit Office).
Framework for Defence
Threat modelling & asset inventory
Data integrity controls
Access isolation
Logging & audit trails
Drift monitoring
Adversarial testing
Rollback plan
Aligned with the EU AI Act’s high-risk obligations: risk management, logging, human oversight (European Commission).
In healthcare, AI isn’t “just software” — it’s safety-critical infrastructure.
Your pacemaker is now an endpoint. Attackers read release notes too.
Why Devices + AI Are Tricky
Firmware–model coupling, edge inference, constrained compute, long lifetimes.
Risks mapped in Biasin et al.’s study on AI medical device cybersecurity (arXiv).
Case in Point
The 2017 firmware recall for ~465k Abbott (St. Jude) pacemakers shows the stakes, a patch was issued to mitigate RF cybersecurity vulnerabilities (Read more).
Regulatory Overlap
AI used for medical purposes typically lands in high-risk under the AI Act, layering obligations on top of MDR/IVDR (European Commission).
This includes logging, robustness, and human oversight.
Secure Design Patterns
Isolation/sandboxing
Secure boot + model integrity checks
Fail-safe fallback modes
Lightweight cryptography
Device logging & anomaly detection
OTA updates with rollback
Adversarial robustness testing
Ship devices with a patch plan, audit trail, and model provenance. Or don’t ship at all.