
Digital Health Commercialisation in Europe: Why the Operating Model Beats the IP
Digital health companies love to talk about defensible technology. European health systems are much less romantic. They care whether the product gets used, fits the workflow, generates evidence, survives procurement and justifies reimbursement after the first enthusiasm fades.
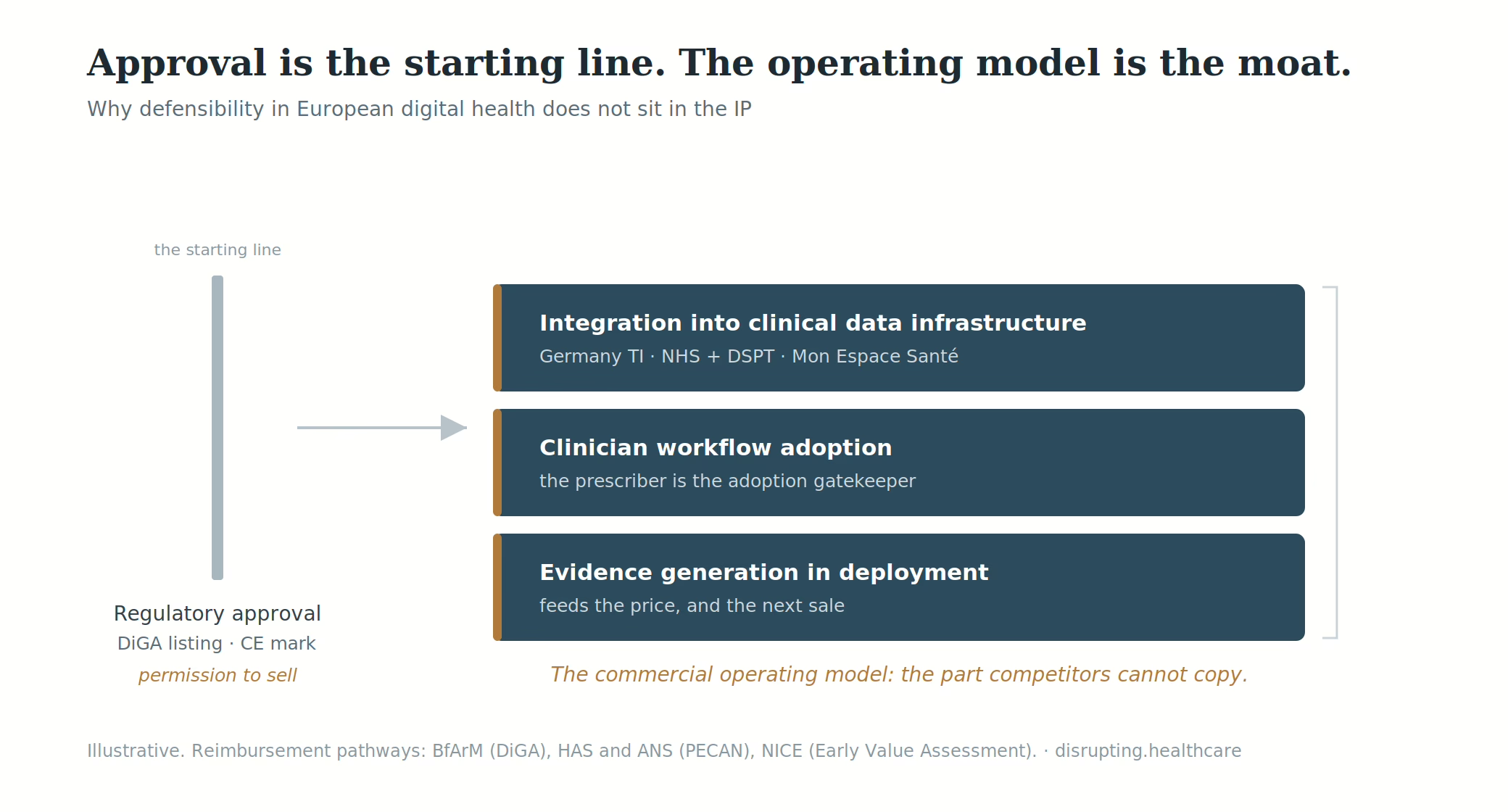
In Europe, a CE mark, a DiGA listing, a PECAN decision or a positive early value signal is not a commercial position. It is permission to attempt one.
The durable advantage is the commercial operating model: the system through which a company integrates into clinical infrastructure, earns clinician trust, generates real-world evidence, manages market-specific reimbursement requirements and compounds learning from one deployment into the next.
That is less glamorous than IP. It is also harder to copy.
A listing is a starting line, not a market position
Germany remains the best place to see the difference between access and adoption because its DiGA pathway is the most mature dedicated digital health reimbursement route in Europe.
The German model is real. BfArM describes DiGA as reimbursable digital health applications that can be prescribed by physicians or psychotherapists, with around 73 million people covered by statutory health insurance entitled to access them. The BfArM fast-track assesses, among other things, technical requirements, data protection, user-friendliness and evidence of a positive healthcare effect. Lower-risk DiGA can be listed provisionally while evidence is generated, usually within twelve months and in exceptional cases up to twenty-four months.
That is a powerful access mechanism. It is not a guarantee of durable commercialisation.
The 2025 report from GKV-Spitzenverband shows the market has moved beyond novelty. Since 2020, 74 DiGA had been admitted to the directory; 16 had already been removed during the trial phase, leaving 58 in the BfArM directory at the end of 2025. By that point, 1.9 million DiGA had been prescribed or approved, 1.6 million had been activated, and statutory health insurance expenditure had reached around €400 million. Usage had grown by 63% compared with the previous year.
So yes, the category is established. And no, that does not mean every listed product has scaled.
The same GKV report notes that 83% of patients who activate a DiGA do not receive a follow-up prescription after the intended use period, usually around 90 days. That number does not make DiGA a failure. It does make one thing obvious: a reimbursement route does not automatically create sustained clinical behaviour. The operating model still has to earn use.
This is the first rule of digital health commercialisation in Europe: access is not adoption. Adoption is built after access, in the messy bit where clinicians, patients, payers, data systems and care pathways meet.
Why IP is a weak commercial moat in European digital health?
IP matters. Of course it does. A differentiated algorithm, validated dataset, user experience, clinical workflow or device-software combination can create defensibility.
But in European digital health, IP rarely does the hardest commercial work alone.
The first weakness is procurement. Hospitals, payers and national health systems do not buy patents. They buy lower pathway friction, credible outcomes, compliance readiness, implementation support and budget logic. A clever algorithm that requires too much behaviour change from clinicians will lose to a less elegant product that fits the clinical day.
The second weakness is reimbursement fragmentation. A product that works commercially in Germany may need a different evidence package, pricing logic and stakeholder model in France. A UK NHS trust may care less about a continental reimbursement badge than about DTAC readiness, data protection, clinical safety, interoperability and local pathway impact.
The third weakness is evidence. Digital health products do not stand still after launch. Models update, workflows change, user populations shift, integrations mature, and clinical claims evolve. That means the evidence story cannot be frozen at regulatory approval. It has to be generated continuously in deployment.
The fourth weakness is trust. Digital health adoption depends on the willingness of clinicians to recommend the product, patients to use it, payers to fund it and healthcare organisations to integrate it. Trust is operational. It is built through support, transparency, implementation quality and evidence loops. A patent does not answer the nurse who says the system adds five minutes to an already impossible workflow.
That is why the operating model becomes the moat.
The three layers that decide commercialisation
The operating model has three load-bearing layers.
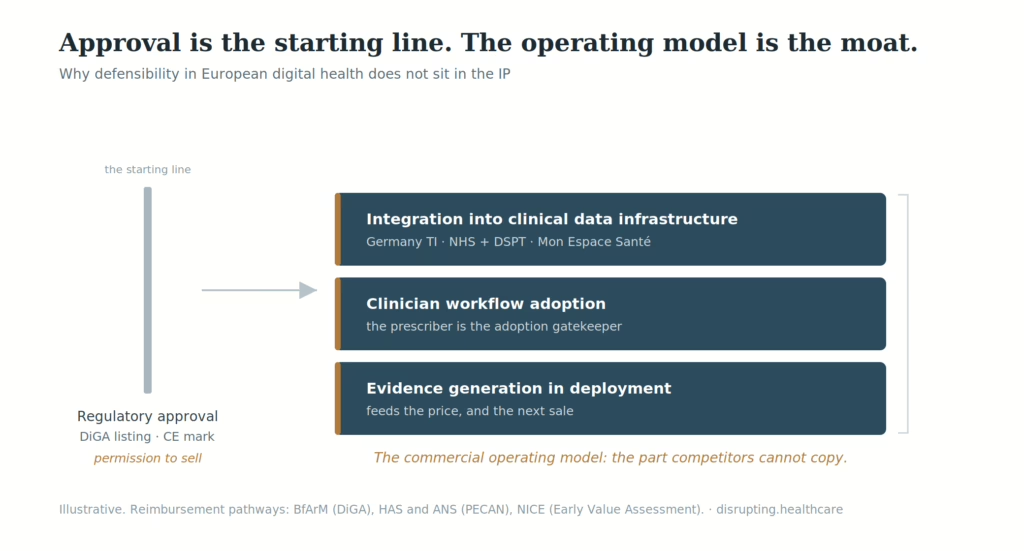
The first is infrastructure integration. In Germany, that means designing around the telematics infrastructure, BfArM requirements, statutory insurance processes and the practical realities of prescription, activation and follow-up. In France, it means working with PECAN or permanent reimbursement routes, interoperability and security requirements, and the broader digital health environment around Mon espace santé. In England, it means understanding NHS procurement, DTAC, data protection, clinical safety and interoperability expectations.
This is not glamorous. It is also where many digital health strategies quietly die. A product that does not fit the systems clinicians already use becomes a side task. Side tasks do not scale.
The second layer is clinician workflow adoption. For digital therapeutics, remote monitoring and decision-support tools, the prescribing or recommending clinician is often the most important commercial variable. Too many companies design around the clinician rather than for the clinician. They secure access, then discover that the product asks too much of the person whose behaviour determines adoption.
The operating-model question is brutally simple: what exactly must change in the clinician’s day for this product to be used, and why is that change worth it?
If the answer is weak, no amount of positioning polish will rescue the launch.
The third layer is evidence generation in deployment. Every live site should become part of the evidence engine: usage, adherence, patient outcomes, pathway impact, clinician feedback, operational friction, economic value, and failure modes. This is no longer a nice additional capability. It is becoming structurally necessary.
Germany is already moving in that direction. The GKV report describes planned mandatory application-accompanying success measurement, including data on duration and frequency of use, patient satisfaction and patient-reported health status, with results expected to be published in the DiGA directory and made available for price negotiations. The direction of travel is clear: digital health companies will increasingly have to prove performance after access, not only before it.
That changes the commercial model. A company that cannot capture, interpret and use deployment evidence is not ready for European scale.
Europe is not one market. Annoying, but true.
European digital health strategy often collapses under one attractive but false assumption: win one national pathway, then scale across Europe.
No. Not like that.
Germany, France and England alone show why the single-Europe plan fails on contact.
Germany’s DiGA pathway is a structured national reimbursement route for qualifying digital health applications. BfArM reviews applications through the fast-track, and products may be permanently listed if the positive healthcare effect is proven or provisionally listed while evidence is generated.
France’s PECAN pathway is different. HAS describes PECAN as a one-year, non-renewable early reimbursement route for presumably innovative digital medical devices, while the company works towards ordinary reimbursement through LPPR or LATM. G_NIUS describes it as one year of exceptional coverage by French national health insurance for sufficiently mature solutions, allowing the operator to finalise the demonstration of clinical or organisational benefits while already being reimbursed.
England is different again. NICE HealthTech guidance evaluates digital technologies, diagnostics and medical devices, including AI. NICE’s early value assessment approach is designed for promising technologies where the evidence base is still developing, with further evidence generation built into the access logic. NHS England’s updated Digital Technology Assessment Criteria, introduced in February 2026 with transition from the previous form by 6 April 2026, focuses DTAC on software-based digital health technologies and reduces duplicative questions while retaining the assurance logic around safe adoption.
Three markets. Three gatekeeping logics. Three evidence rhythms.
The companies that scale in Europe do not translate a single go-to-market plan. They sequence markets deliberately, build the specific operating infrastructure each market requires, and reuse only what is genuinely portable: evidence principles, implementation playbooks, health-economic logic, product learning and governance.
One visible warning sits in France. HelloBetter Insomnie, from a German digital therapeutics provider, received an unfavourable CNEDiMTS opinion for PECAN early coverage in 2024. The product’s German pedigree did not make French early reimbursement automatic. That is exactly the point. European digital health scale is not a passport-stamping exercise.
What investors are now underwriting?
The capital market has learned the same lesson, albeit after burning a ceremonial amount of money.
Galen Growth’s 2025 analysis describes a market moving from hype to measurable results, with investors prioritising validated endpoints, clinical ROI and scalable outcomes rather than untested algorithms. Its Q3 2025 European digital health analysis found that two-thirds of total funding went to growth-stage ventures, signalling a preference for companies with demonstrable clinical impact.
That shift matters for founders and corporate partners. The story investors want is no longer simply: we have technology, regulatory clearance and a large addressable market. The stronger story is: we know which market we are entering first, which stakeholder behaviour must change, what evidence is required, how we support implementation, how we measure outcomes, and how that evidence improves the next commercial conversation.
In other words, investors are underwriting the operating model.
The EU itself is also trying to address Europe’s scale-up problem. The European Innovation Council’s Scaleup Europe Fund is explicitly designed to help Europe boost investments in scaleups and close the gap with global leaders. That helps. But capital alone does not fix fragmentation. A larger cheque will not make PECAN behave as DiGA, or an NHS buyer behave like a German statutory insurer.
For European digital health, capital is useful only when it funds the boring capabilities that scale: HEOR, clinical implementation, integration, regulatory intelligence, market access, customer success and real-world evidence.
Yes, I know. Less sexy than “AI-native platform”. Also more likely to survive procurement.
What a serious European commercial operating model includes?
A serious operating model for digital health commercialisation in Europe has six components.
First, market sequencing. Pick the first two markets because the reimbursement logic, evidence requirements, infrastructure readiness and commercial learning compound. Do not pick them because a board slide looks prettier with more flags.
Second, clinical implementation. Treat the signed contract or reimbursement decision as the beginning of adoption, not the end of sales. Implementation should include workflow mapping, training, patient onboarding, clinical support, escalation logic and usage monitoring.
Third, evidence generation. Build evidence capture into deployment from day one: utilisation, persistence, outcomes, patient-reported measures, clinician feedback, pathway impact and economic value. If evidence collection begins only when renewal or price negotiation approaches, the operating model is already late.
Fourth, health economics. HEOR cannot be an occasional outsourced deck. It has to inform product design, target market choice, pricing, payer argumentation and real-world evidence priorities.
Fifth, integration capability. Digital health is only digital in the investor pitch. In the hospital, it is a workflow and infrastructure problem. Integration with electronic records, national digital health platforms, identity, security, data flows and clinical systems is commercial infrastructure.
Sixth, regulatory and policy intelligence. MDR, the EU AI Act, EHDS, national reimbursement reforms, cybersecurity expectations and procurement rules are not background noise. They change market timing, commercial risk, evidence expectations and the cost of scale.
This is where many digital health companies discover that commercialisation is not a sales function. It is a system.
Neko Health’s $700 million Series C provides a current test of whether a European company can scale an integrated technology, clinic, evidence and membership model internationally.
What corporate partners should look for?
Pharma, MedTech and diagnostics companies looking at digital health partnerships should also change their due diligence.
The lazy version asks: is the product differentiated, does it have regulatory clearance, and can it support our brand or pathway strategy?
The better version asks: where has it been implemented, what changed in the clinical workflow, what usage persisted after launch support faded, what evidence was generated in live deployment, what reimbursement pathway has it survived, what integration work was required, and what did the company learn from the first failed deployment?
That last question is underrated. Digital health companies that have never failed in implementation may simply not have implemented enough.
For pharma, the strategic value of digital health often sits around adherence, diagnosis, monitoring, patient support, pathway redesign and real-world insight. For MedTech, it sits around connected care, service models, remote monitoring, workflow efficiency and evidence beyond the device. In both cases, the partner’s operating model matters more than the demo.
A product can look excellent in a pilot and still be commercially immature. The difference is whether the company can turn adoption into a repeatable system.
One Thing To Remember